Background: Direct oral anticoagulants (DOACs) provide a safe and effective alternative to vitamin K antagonists (VKAs) for treatment of venous thromboembolism (VTE), as shown in a previous intention-to-treat comparative effectiveness analysis. However, on-treatment analysis is imperative in observational studies because the duration and choice of anticoagulation is at the investigators’ discretion.
Aims: Compare the effectiveness of DOACs and VKAs on 12-month outcomes in VTE patients using on-treatment analysis.
Methods: GARFIELD-VTE (ClinicalTrials.gov: NCT02155491) is a global, prospective, non-interventional study of real-world treatment practices. This on-treatment analysis included 8,034 patients treated with either VKA (n=3,043, 37.9%) or DOAC (n=4,991, 62.1%), with or without parenteral anticoagulation bridging. The causal treatment effect was estimated using marginal structural models with inverse probability weights to account for the time-varying nature of exposure and confounders, and to correct for the effect of major bleeding on dropout.
Results: After adjustment for baseline characteristics, all-cause mortality was significantly lower with DOACs than with VKAs (hazard ratio [HR]: 0.58; 95% confidence interval [CI] 0.42-0.79, p=0.001) (Figure 1). Patients receiving VKAs were more likely than those receiving DOACs to die of VTE complications (4.9% vs. 2.2%) or from bleeding (4.9% vs. 0.0%). There was no significant difference in recurrent VTE (HR: 0.74, 95% CI 0.55-1.01), major bleeding (HR: 0.76, 95% CI 0.47-1.24), or overall bleeding (HR: 0.87, 95% CI 0.72-1.05) with DOACs or VKAs (Table 1). VTE patients with active cancer were more likely to die if they received a VKA than a DOAC (52.51 [37.33-73.86] vs 26.52 [19.37-36.29] per 100 person-years, respectively). This was also true for VTE patients with concomitant renal insufficiency (9.97 [7.51-13.23] vs 4.70 [3.25-6.81] per 100 person-years, respectively).
Conclusions: With similar rates of recurrent VTE and major bleeding, DOACs were associated with reduced rates of all-cause mortality and a lower likelihood to die from VTE or fatal bleeding compared to VKAs.
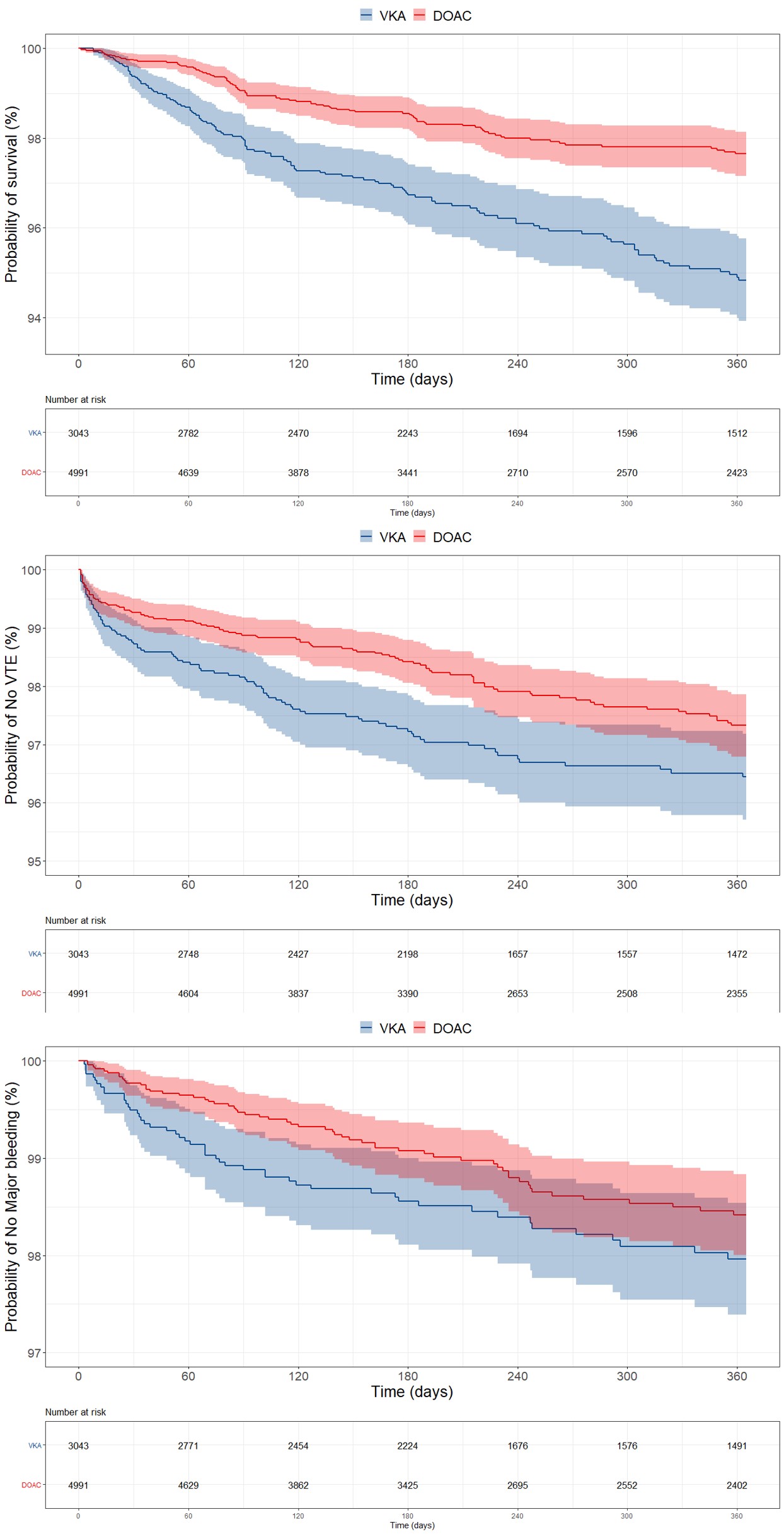 Kaplan-Meier curves for all-cause mortality, recurrent VTE and major bleeding in VTE patients receiving oral anticoagulants. Abbreviations; DOAC: direct oral anticoagulant, VKA: vitamin K antagonist, VTE: venous thromboembolism
Kaplan-Meier curves for all-cause mortality, recurrent VTE and major bleeding in VTE patients receiving oral anticoagulants. Abbreviations; DOAC: direct oral anticoagulant, VKA: vitamin K antagonist, VTE: venous thromboembolism
| Outcome | VKA | DOAC | Adjusted* HR | 95% CI | P-value | ||
| Event rate | 95% CI | Event rate | 95% CI | ||||
| All-cause mortality | 5.69 | 4.76-6.79 | 2.61 | 2.12-3.20 | 0.58 | 0.42-0.79 | 0.001 |
| Recurrent VTE | 4.32 | 3.52-5.30 | 2.97 | 2.44-3.61 | 0.74 | 0.55-1.01 | 0.058 |
| Major bleeding | 2.35 | 1.78-3.10 | 1.69 | 1.30-2.18 | 0.76 | 0.47-1.24 | 0.27 |
| Any bleeding | 12.65 | 11.20-14.29 | 12.02 | 10.89-13.26 | 0.87 | 0.72-1.05 | 0.151 |
| Myocardial infarction/ACS | 0.56 | 0.32-0.99 | 0.44 | 0.26-0.72 | 1.07 | 0.48-2.38 | 0.865 |
| Stroke/TIA | 0.37 | 0.19-0.75 | 0.61 | 0.40-0.93 | 1.57 | 0.53-4.66 | 0.416 |
Incidence rates (per 100 person-years) and adjusted hazard ratios for VTE patients receiving oral anticoagulants. Event rates are shown per 100 person-years. HR values <1 favour DOAC treatment. *HRs were adjusted for major bleeding and dropout at follow-up in addition to the following baseline characteristics: age, gender, ethnicity, BMI, previous aspirin usage, VTE type, site of DVT, care setting, physician specialty, treatment funding source, country, creatinine clearance, active cancer, recent bleeding or anaemia, pregnancy or postpartum, family history of VTE, history of cancer, known thrombophilia, prior VTE episodes and renal insufficiency. Abbreviations; CI: confidence interval, DOAC: direct oral anticoagulant, VKA: vitamin K antagonist, VTE: venous thromboembolism, ACS: acute coronary syndrome, TIA: transient ischemic attack
To cite this abstract in AMA style:
Haas S, Bounameaux H, Farjat AE, Ageno W, Weitz JI, Goldhaber SZ, Turpie AGG, Goto S, Angchaisuksiri P, MacCallum P, Ten Cate H, Panchenko E, Carrier M, Sanchez Dias CJ, Gibbs H, Jansky P, Kayani G, Schellong S, Prandoni P, Kakkar AK, on behalf of the GARFIELD-VTE investigators . Comparative Effectiveness of Oral Anticoagulants in Venous Thromboembolism: On-treatment Analysis in GARFIELD-VTE [abstract]. Res Pract Thromb Haemost. 2021; 5 (Suppl 2). https://abstracts.isth.org/abstract/comparative-effectiveness-of-oral-anticoagulants-in-venous-thromboembolism-on-treatment-analysis-in-garfield-vte/. Accessed May 19, 2024.« Back to ISTH 2021 Congress
ISTH Congress Abstracts - https://abstracts.isth.org/abstract/comparative-effectiveness-of-oral-anticoagulants-in-venous-thromboembolism-on-treatment-analysis-in-garfield-vte/